GLAUCOMA FAQs
What is Glaucoma?
Can Glaucoma be treated?
How is Intraocular Pressure (IOP) involved?
What are the Risk Factors For Developing Glaucoma?
Do All People With High IOP Get Glaucoma?
Why Is Corneal Thickness Relevant?
Do Patients With Glaucoma Always Have High IOP?
Is Treatment Different For Normal Tension Glaucoma?
What Kind Of Glaucoma Do I Have?
What Should I Expect When I Attend the Glaucoma Clinic?
SURGICAL OPTIONS
Trabeculectomy
Tube/Shunt
Non-Penetrating
OTHER PROCEDURES
New Procedures
Revision Procedures
What Kind Of Glaucoma Do I Have?
Glaucoma is usually divided into open angle and closed angle forms.
To understand about the angle and its relevance to IOP click here
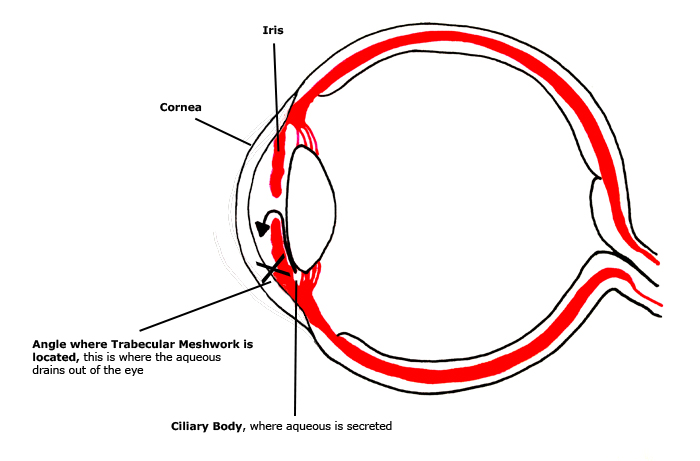
If the angle is narrow, or closed (in other words the edge of the iris touches the edge of the cornea), then it is difficult for the aqueous to leave the eye, so IOP will go up.
When the angle is closed, patients are described as having angle closure, whether or not the pressure is high. If the angle is closed and there are features of glaucoma damage in the optic nerve then the patient has angle closure glaucoma.
Open Angle
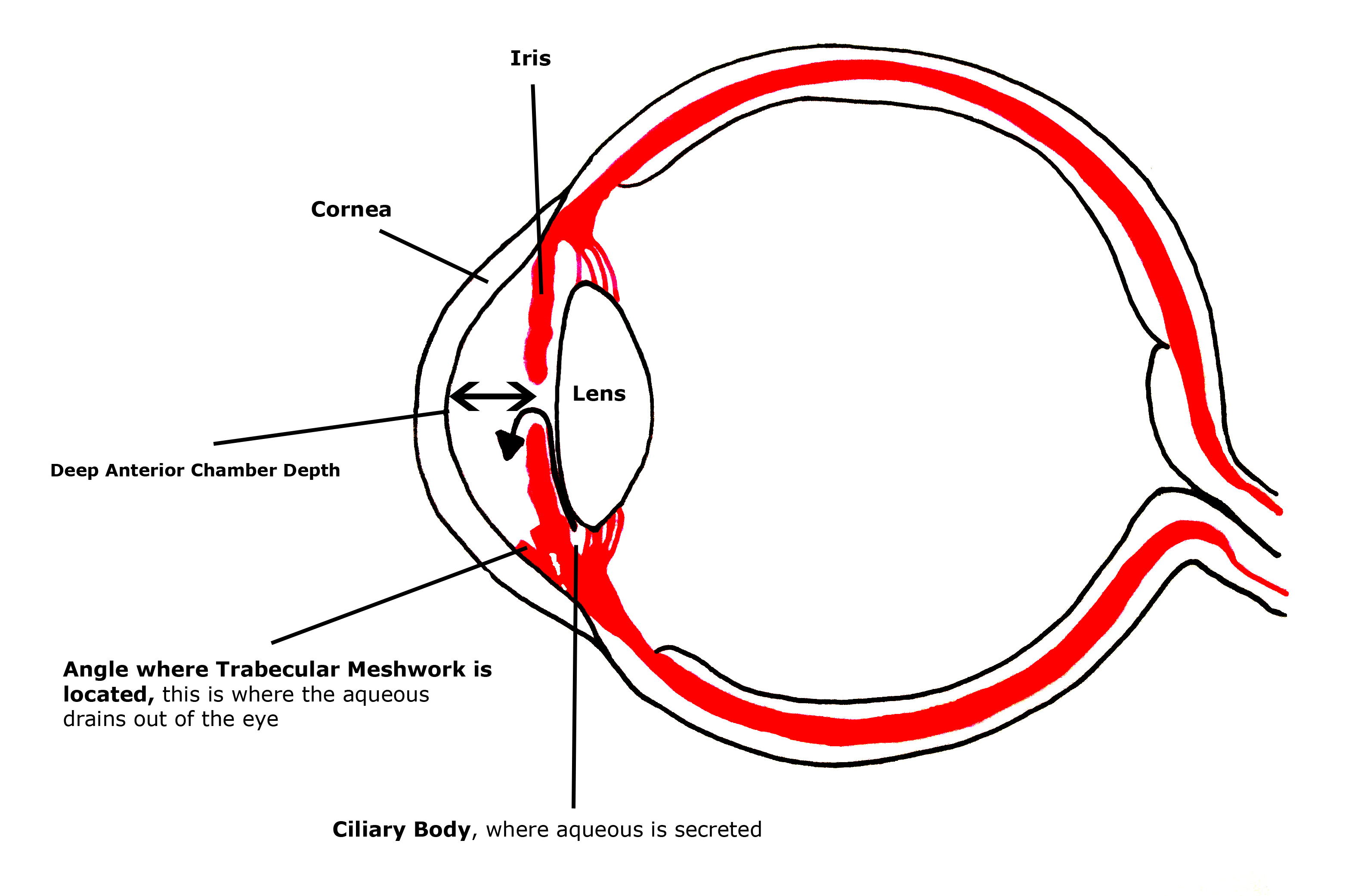
Most glaucoma cases in the UK have an open angle. In these cases it is assumed that the high pressure is caused by problems in the trabecular meshwork that cannot be seen with the naked eye.
Primary and Secondary Glaucomas
Glaucoma is further divided into primary and secondary forms.
Secondary
Secondary means that the high pressure or angle closure is caused by some other medical factor. There are secondary open angle problems and secondary angle closure problems.
Common causes of secondary glaucoma include:
• High IOP after vitreo-retinal surgery
• High IOP after corneal surgery
• High IOP following the use of steroids
• High IOP following uveitis (inflammation) in the eye
With secondary glaucomas, the underlying cause will need to be treated, as well as the high IOP. Often the treatment for secondary glaucomas is surgical as the pressures can be very high and sight may be threatened over a short space of time. For further information regarding secondary glaucomas, click here
Primary
Primary means that there is no identifiable underlying cause for the glaucoma or of the high pressure. In the UK, the most common cause of glaucoma is primary open angle glaucoma.
There are two relatively common risk factors for developing glaucoma with an open angle. These are called pigment dispersion syndrome and pseudoexfoliation. These risk factors are common enough that they are often classed together with primary open angle (called chronic open angle glaucoma in the NICE guidance).
Pigment dispersion syndrome (PDS)
PDS occurs when pigment from the back of the iris is shed and the granules of pigment block the trabecular meshwork, causing the IOP to go up.
In some patients, the pressure can go extremely high particularly after periods of intense exercise when pigment shedding is increased.
When the high IOP causes glaucomatous optic nerve damage, it is called pigmentary glaucoma.
PDS is more common in men in their 30-40s with myopia (short-sightedness).
Occasionally, pigment dispersion can occur as a secondary complication from cataract surgery.
Pseudoexfoliation (PXF)
PXF is caused by a type of fibrillar material that is deposited throughout the eye (and indeed the rest of the body), in particular on the surface of the lens.
PXF material is shed from the lens and this can 'clog up' and damage the trabecular meshwork, increasing the IOP leading to glaucoma.
When there is glaucomatous optic nerve damage, it is called pseudoexfoliative glaucoma.
PXF occurs in all races, but is perhaps more common in Scandinavian and Southern Mediterranean races.
The treatment of ocular hypertension and glaucoma due to pseudoexfoliation or pigment dispersion is the same as for other forms of ocular hypertension and glaucoma.